If a healthcare employer says “medical coding”, are they talking about the same job as “clinical coding”?
Sometimes, but not usually in the way most readers expect.
That is where the confusion begins. On the surface, the two phrases sound interchangeable. In practice, they often point towards different settings, different systems, and different career paths. Typically, one term leads towards the formal NHS hospital route. Meanwhile, the other is more often used more loosely, especially in GP practices, primary care, and record-coding roles built around patient data systems rather than hospital episode coding.
That distinction matters much more than it seems. It affects the kind of work you apply for, the coding systems you need to learn, the training route that makes sense, and even the long-term direction of your career. If you misunderstand the wording early on, it becomes very easy to choose the wrong course, chase the wrong vacancies, or assume one branch of healthcare coding is the same as another when it is not.
For that reason, this article does not treat Clinical Coding vs Medical Coding as a small wording debate. Instead, it treats it as a practical job-search question. If you want to understand what employers usually mean, where the lines overlap, and which term matters most for the route you actually want, this is the comparison that clears things up.
Same Theme, Different Job
At first glance, Clinical Coding vs Medical Coding looks like one of those technical phrases that different people use in different ways. That is partly true, but it is not the whole story.
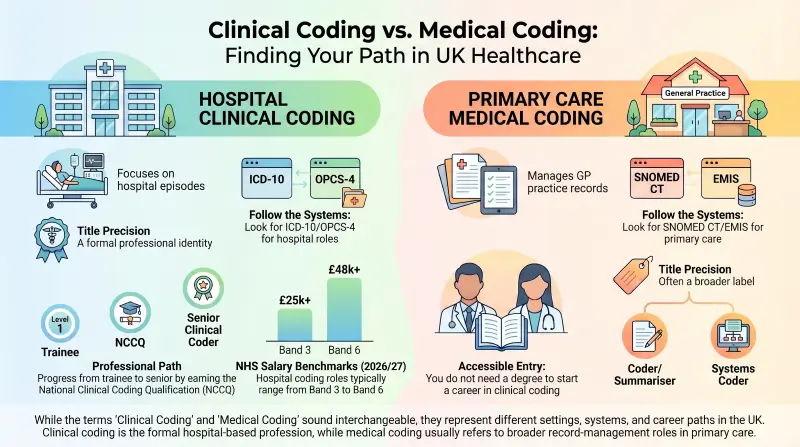
In real healthcare recruitment, the wording often signals a difference in setting. Clinical coding usually points towards the formal hospital-based profession linked to admitted patient care, classifications such as ICD-10 and OPCS-4, national coding standards, and a recognised progression route. Medical coding, by contrast, often appears in broader record-coding roles, especially in general practice and primary care, where the work is more likely to involve structured data entry, coded correspondence, summarising, and systems such as SNOMED CT and EMIS.
That does not mean there is a hard wall between the two. Employers do not always label jobs perfectly. Some adverts use “clinical coder” for primary care work. Some course providers use “medical coding” because it is a familiar search phrase. Some readers use both terms because they have seen both online. But once you look at the job setting and the systems mentioned, the picture becomes much clearer.
So the key idea is this: the terms overlap, but they do not point to the same thing often enough to treat them as identical.
Why the Two Terms Get Mixed Up So Easily
Part of the confusion comes from search behaviour. Many readers first meet this topic through broad internet searches, and a lot of online content around coding careers comes from outside Britain. In those markets, medical coding is the standard phrase, so readers naturally bring it into their own search journey and assume employers use it the same way here.
Then they open job ads and find something different. Hospital roles usually use the language of clinical coding, while primary care roles may switch between medical coder, clinical coder, coder/summariser, or even clinical systems coder, depending on the employer. That makes the field look far more blurred than it really is.
The second reason is that healthcare does not use one single coding method everywhere. Hospital coding relies on classifications designed for diagnoses and procedures. Primary care relies much more heavily on structured clinical terminology inside patient-record systems. To an outsider, both look like “coding healthcare records”. To an employer, they can mean very different day-to-day work.
The third reason is that titles often travel further than responsibilities. Readers remember the headline first. Employers, however, usually tell the truth deeper in the advert. The system name, the kind of records involved, the qualification mentioned, and the setting itself often reveal more than the title ever will.
What Clinical Coding Usually Means
When employers talk about clinical coding in the more formal sense, they are usually talking about hospital coding. This is the branch that sits inside acute trusts and coding departments, where coders translate diagnoses and procedures from patient records into recognised classifications used for reporting, analysis, reimbursement, audit, and service planning.
That is why the role has a more defined professional identity than many people realise. It is not simply administrative coding. It is tied to national standards, hospital activity data, and a recognised training path. For that reason, the formal qualification route matters so much here. If your goal is to become a hospital clinical coder, the job title is part of a bigger professional framework rather than a loose label.
In practical terms, this side of the field is closely associated with:
- ICD-10 for diseases and health conditions.
- OPCS-4 for interventions and procedures.
- Inpatient and day-case activity.
- Coding departments within hospitals.
- Progression towards the NCCQ and related specialist roles.
This is the world most people are referring to when they ask about the clinical coder role, clinical coding training, or how clinical coding works in the NHS.
More Than an Office Task
One reason hospital clinical coding is often misunderstood is that it sounds quieter than it really is. Yes, it is office-based. Yes, it is detailed. But it is not passive work.
A hospital coder has to read complex records, identify what is clinically significant, follow rules properly, and work with documentation that is not always neat or complete. The job depends on accuracy, judgement, and consistency. That is why it attracts people who enjoy detail, structure, and information work with a clear purpose behind it.
What Medical Coding Usually Means in Job Ads
Now look at the other side.
When employers use medical coding in job ads, they are often referring to primary care coding, patient-record coding, or summarising work rather than hospital episode coding. These jobs tend to sit inside GP surgeries, practices, and other community-based settings where the focus is on keeping patient records accurate, structured, searchable, and useful for clinical and administrative work.
That usually means coding incoming correspondence, updating diagnoses in the record, maintaining chronic disease registers, supporting reporting tasks, and working inside systems such as EMIS. The skill set still includes accuracy, terminology, and careful data handling, but the context is different. The work is often closer to structured record management than to the formal hospital coding profession.

This is why the phrase medical coding meaning can feel so vague when people first search it. It exists, but it often acts as a wider umbrella rather than a tightly defined hospital title. In one setting, it may mean coding and summarising in a GP surgery. In another, it may be a marketing phrase on a course page. In a third, it may be used by an employer who is not particularly strict about the distinction.
The Important Point
The phrase is real, but it is often less precise. So if you see medical coding jobs advertised, do not assume they match the classic hospital clinical coding pathway. Read further. The title may be broad, but the systems, tasks, and employer setting usually make the difference obvious.
The Systems Tell the Real Story
If job titles create confusion, systems create clarity. One of the easiest ways to understand the difference between clinical coding and medical coding is to stop staring at the title and look at the terminology in the advert.
| Setting | Title You May See | Systems or Standards Mentioned | What the Work Usually Supports |
|---|---|---|---|
| Hospital coding departments | Clinical Coder, Trainee Clinical Coder, Senior Clinical Coder | ICD-10, OPCS-4, national coding standards, PAS, encoder systems | Inpatient coding, procedures, reimbursement, audit, casemix, hospital reporting |
| GP or primary care settings | Medical Coder, Clinical Coder, Coder/Summariser, Clinical Systems Coder | SNOMED CT, EMIS, coded correspondence, QOF, summarising | Primary care record quality, coded data capture, workflow support, and reporting |
This is where many readers finally see the difference clearly. The same broad theme appears on both sides, but the systems reveal two different branches of work.
When you see ICD-10 and OPCS-4, you are usually looking at the formal hospital path. In contrast, seeing SNOMED CT and EMIS usually means you are looking at primary care record coding.
For this reason, not every course that says “medical coding” points neatly towards a hospital coding career. Sometimes it is aimed at the primary care side. Sometimes it uses wider wording to attract broader searches. Sometimes it is simply not very clear.
How the Day-to-Day Work Changes
This is the point many comparison articles skip, even though it is where the difference becomes real.
A hospital clinical coder is more likely to spend the day working through admitted patient records, operation notes, discharge summaries, diagnoses, complications, and procedure details. The job often involves handling more complex, speciality-based documentation and ensuring the coded outcome matches the patient episode correctly under recognised standards.
A primary care medical coder, on the other hand, is more likely to work with incoming letters, test results, summaries, diagnoses already flowing into the patient record, and structured coding inside the practice system. The work may include summarising records for new patients, coding correspondence, supporting registers, and helping the surgery keep its data accurate and useful.
They both require concentration. Careful handling of sensitive information is also essential. But they do not feel the same in practice.
A Quick Contrast
Hospital clinical coding usually feels more like:
- Classification-driven coding.
- Speciality-based record interpretation.
- Coding episodes of care.
- Formal standards-led work.
Primary care medical coding usually feels more like:
- Record maintenance and coded updates.
- Terminology-led data capture.
- Correspondence coding and summarising.
- Practice-system accuracy and workflow support.
That difference in rhythm matters. One route is usually built around admitted care and clinical classifications. The other is often built around maintaining high-quality structured records in practice systems.
Does the Wording Change the Career Path?
Yes, and this is one of the most useful things to understand early.
If you step into the hospital clinical coding route, you are entering a career path with more visible progression. The route usually starts with trainee or junior roles, then develops through experience, standards knowledge, and movement towards the National Clinical Coding Qualification. From there, people can progress into senior coding, speciality-based work, audit, training, and supervisory roles.
If you step into a primary care medical coding role, the direction can be different. It may still lead to valuable experience and a solid healthcare data career, but the ladder may move more towards records management, data quality, systems work, workflow support, or broader administration in general practice rather than the hospital coding profession.
That does not make one route “better” in every case. It means they are different choices.
Why This Matters for Learners
A lot of beginners search for a medical coding course, thinking it will lead straight into hospital clinical coding. Sometimes it may help them build useful foundations. Sometimes it may not align well at all.
So the smarter question is not just, “Which course sounds good?” It is, “Which branch of healthcare coding am I actually preparing for?”
Salary and Progression: Why the Wording Can Change the Path
Salary is one of the topics strong-ranking pages nearly always cover, and readers expect it here too. The difference is that, for this topic, salary only matters if it helps explain the route.
Hospital clinical coding salary is easier to track because it usually sits within clearer structures. Trainee and senior hospital coding roles often follow familiar NHS banding patterns, so progression is easier to understand. That gives this branch of the field a more visible career ladder.
Primary care coding roles can still pay well for the right candidate, but the structure is often less standardised. Pay may vary more between employers, practices, and levels of responsibility. So if someone thinks they are applying for a hospital coding career but lands in a very different kind of practice-based records role, they may find that the progression picture looks different, too.
That is why the wording in the advert can quietly shape the route you end up following. The title does not just affect your search results. It can affect your longer-term direction.
How to Read a Coding Job Ad Properly
If you want to avoid confusion, do not stop at the headline. Instead, scan for the clues that tell you what the role really is.
Watch for These Signals
If the advert mentions the following, it usually points towards the hospital clinical coding route:
- ICD-10.
- OPCS-4.
- Admitted patient activity.
- Coding standards.
- Hospital specialities.
- Trainee clinical coder or senior clinical coder language.
If the advert mentions the following, it is more likely to be a primary care or practice-based coding role:
- SNOMED CT.
- EMIS.
- Coded correspondence.
- Summarising.
- QOF.
- Surgery or practice workflows.
That habit alone can save a lot of wasted time. Readers often feel confused because they are comparing job titles when they should be comparing employer context.

So Which Term Matters More?
If the question is which phrase carries more formal weight in healthcare recruitment, the answer is clinical coding. That is the term more closely tied to the recognised hospital route, structured training, and specialist progression.
If the question is whether medical coding is still used, the answer is yes. It appears in real job ads and real course marketing, but usually in a broader, less tightly defined way. Very often, it points towards primary care record coding rather than the classic hospital profession.
So the cleanest conclusion is this:
Clinical Coding vs Medical Coding is not a meaningless wording difference. It is often the difference between two branches of healthcare data work that overlap in theme but not always in purpose.
Understand the setting, and the wording starts to make sense.
Get valuable training, UK-focused support, and the skills employers want. No experience needed.
Join 50+ graduates who landed tech jobs with our industry-focused training programme designed for beginners.
Explore Now - Our Job Ready ProgrammeFrequently Asked Questions (FAQs)
Is Clinical Coding the Same as Medical Coding?
Not exactly. Clinical coding usually refers to the more formal hospital-based role linked to ICD-10, OPCS-4, and national coding standards. Medical coding is often used more loosely, especially in primary care and record-management settings.
What Is a Clinical Coder?
A Clinical Coder reads patient notes and medical records, then translates diagnoses and procedures into standardised codes. In hospital settings, this supports reporting, audit, service planning, research, and reimbursement.
How Do I Become a Clinical Coder?
The most common route is to start in a trainee or entry-level role, build knowledge of medical terminology, anatomy, ICD-10, and OPCS-4, then progress through structured workplace training towards recognised qualification.
Which Qualification Matters Most for Clinical Coding?
For the formal hospital pathway, the most important qualification is the National Clinical Coding Qualification (NCCQ). It is the recognised benchmark for progression in NHS clinical coding.
Do I Need a Degree to Start Clinical Coding?
No. You do not usually need a degree. Clinical coding is a route people can enter through training, development, and apprenticeship-based learning rather than a traditional clinical degree.
How Much Do Clinical Coders Earn?
In England, NHS pay provides the clearest benchmark. For 2026/27, Band 3 is £25,760 to £27,476, Band 4 is £28,392 to £31,157, Band 5 is £32,073 to £39,043, and Band 6 is £39,959 to £48,117.
Will AI Replace Clinical Coders?
AI may reshape parts of healthcare coding, but it has not removed the need for skilled human coders. Clinical coding still depends on standards, interpretation, terminology, and quality checks, especially in complex cases.




All Courses
Personal Development
Employability
Career Bundle
Management
Free QLS Certificate
IT & Software
Business
Technology
Health & Care
Quality Licence Scheme Endorsed Courses
Health & Safety
Training
Marketing
Job Ready Programme
Design
Accounting & Finance
Health and Fitness
Healthcare and Medical
Animal Care
Psychology
Microsoft Office
Teach & Education
I.T
HR and Leadership
Counselling and Therapy
Teaching & Child Care
Health and Social Care
Electrical & Electronics
Law
Food Nutrition
programming
Administration & Office Skills
Accounting
Education
Engineering
Cooking & Baking
Language
Law & Criminology
QLS Bundle
Office Skills
Photography
Awareness
Finance
Diet and Nutrition
Lifestyle
Makeup & Beauty
Therapy
Accounting & Bookkeeping
Sports
Mathematics
First Aid
Web Design
Excel
Diet and Fitness
Agriculture
Counselling
General Education
Biotechnology
Networking & Design
Economics
Audit
Lifestyle & Recreational
Adobe Photoshop
Travel and Tourism
Categories

Awarded By

